Patient · Caregiver · Provider Workflows
Designing for Care,
Not Just Compliance
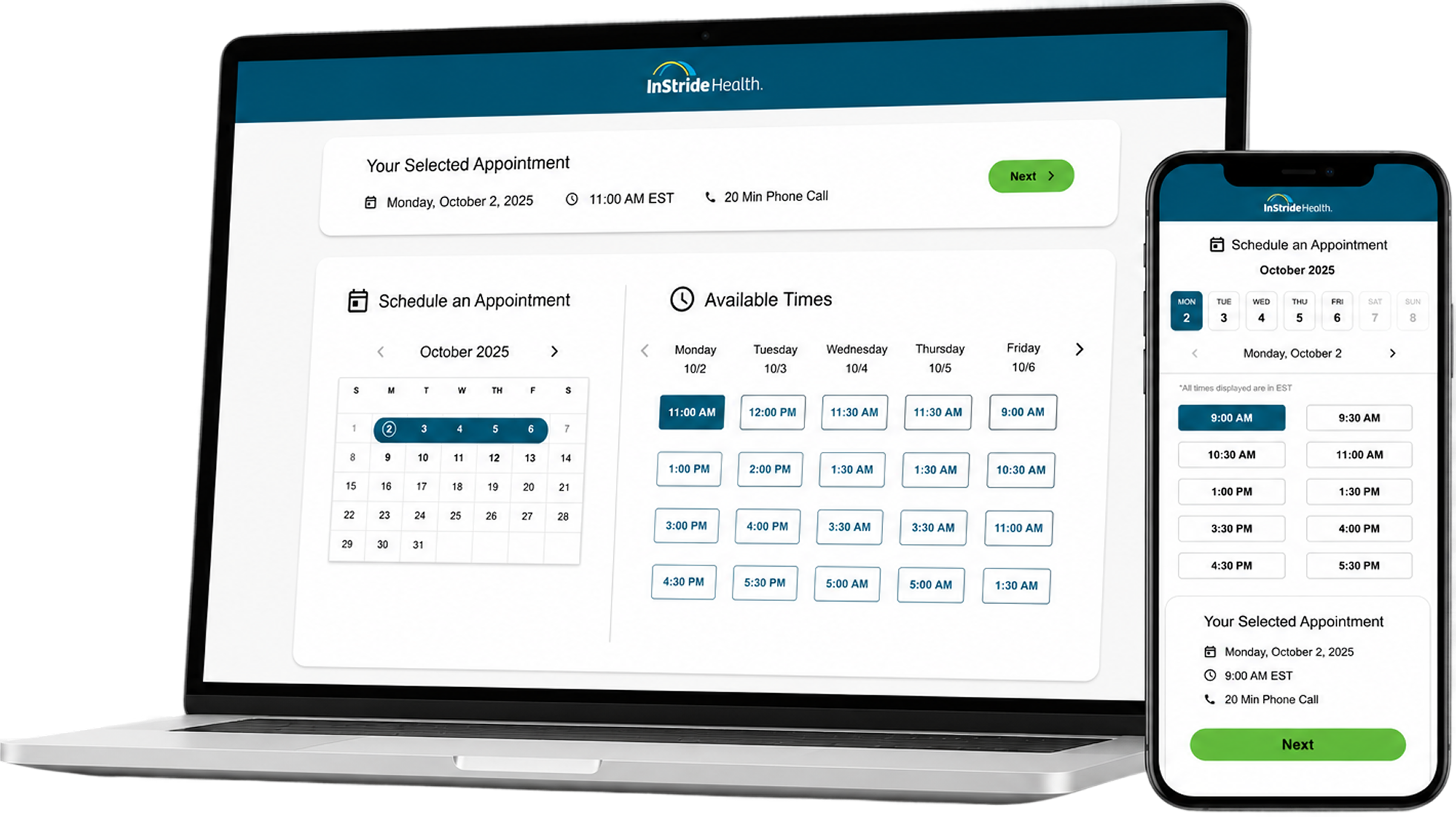
Redesigning a behavioral health app where patients, caregivers, and care teams were all looking at the same information — and drawing completely different conclusions from it.
Three people. One app. Three different realities.
Patients, caregivers, and providers were often looking at the same information—but drawing completely different conclusions from it. A missing assignment might look like procrastination to a caregiver, disengagement to a provider, and simply "I'll do it later" to a patient. The breakdown wasn't missing information. It was a lack of shared understanding.